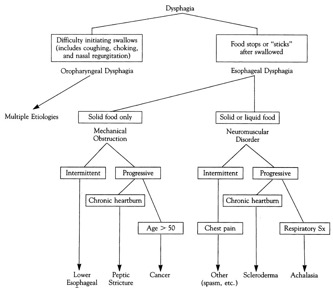
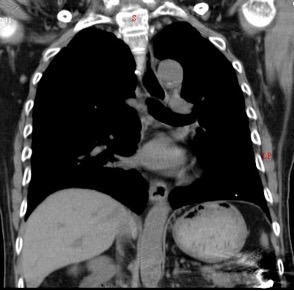
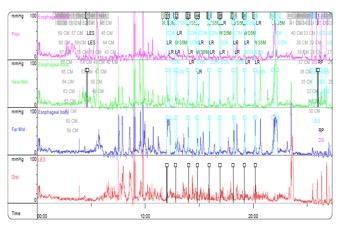
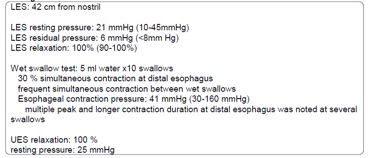
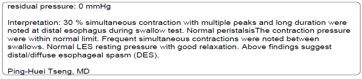
Several examinations were performed per guideline (Algorithm 1). EGD showed gastritis and reflux esophagitis, grade A by LA classification with no luminal stenosis or extrinsic tumors. High esophageal wall tension and spiraling was noted throughout the esophagus. Barium esophagogram (figure 3) was then scheduled to evaluate possible esophageal motility disorder. Result showed corkscrew appearance with partial obstruction, which highly suggested esophageal motility disorders. To exclude secondary cause, Chest CT (figure 4) was arranged and showed only mild wall thickening at lower esophagus. For confirmative diagnosis, esophageal manometry (figure 5) was done under our arrangement, and measurement reports showed simultaneous contraction(>20% wet swallows), intermittent peristalsis, repetitive contraction(>3 peaks), and contraction duration> 6 secs. Results satisfy the conventional manometry criteria for diagnosis of diffuse esophageal spasm (table 2).
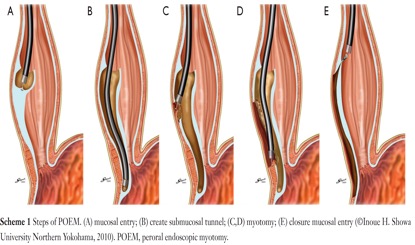
Several medications were prescribed, including smooth muscle relaxants (isosorbide-dinitrate, calcium channel blocker), low dose anti-depressant (sulpiride), proton pump inhibitor (esomeprazole). Exercise and lifestyle modifications were also recommended. However, patient did not experience significant improvement in symptoms. Patient was offered a chance for a new form of treatment. After detailed explanations of risks and benefits, the patient accepted a new kind of sumucosal tunneling technique: Per-Oral Endoscopic Myotomy (P.O.E.M.) (figure 6) characterized by minimal invasive myotomy. Complications during procedure included pneumoperitoneum, pneumomediastinum and pneumoscrotum. Due to these intra-procedure complications, myotomy was only 80% completed. After the procedure, patient was transferred to ICU. Repeat EGD and esophagogram were checked and showed no esophageal mucosal tear or contrast leakage. After monitoring for several days, patient was discharged smoothly. Patient experienced much improvement in symptoms after the procedure.

Primary esophageal motility disorder |
Neuromuscular dysfunction of dysphagia |
Conventional Manometry Criteria |
Achalasia |
Impaired LES relaxation and distal aperistalsis |
Absent distal peristalsis; Relaxation LES pressure < 8mmHg;Rest LES pressure < 45mmHg |
Diffuse esophageal spasm |
Normal contractions, but uncoordinated, simultaneous propagated |
Simultaneous contractions (≥ 20% wet swallows); Intermittent peristalsis; Repetitive contractions(≥ 3 peaks); Duration> 6seconds |
Hypertensive peristalsis (Nutcracker esophagus ) |
Excessive contractions, but a coordinated manner |
Increased distal amplitude (mean pressure >220 mmHg); increased distal peristalsis duration (mean >6 sec) |
義大醫院‧總機電話:07-615-0011‧07-952-0011 地址:82445高雄市燕巢區角宿里義大路1號
語音‧人工掛號專線:07-615-0900‧07-615-0911 週一至週五 07:30~16:30 週六 07:30~11:30
© Copyright 2014. "EDAGI" All rights reserved.